The framework gives us a way of looking at the concepts of health and disability. It acknowledges that every human being can experience a decrease in health and thereby experience some disability. It is not something that happens only to a minority of people. The ICF thus “mainstreams” disability and recognizes it as a widespread human experience. By shifting the focus from the cause to the impact of a health condition, the ICF places all health conditions on an equal footing, allowing them to be compared.
You might wonder why we need a framework to understand a health condition. As I became more familiar with the ICF, I could really see its usefulness. The idea that every human being can experience a decrease in health and therefore experience some disability is useful because it illustrates that people don’t fit neatly into one of two boxes (metaphorically speaking), healthy or disabled. There is, rather, a continuum between health and disability. The framework is helpful because it focuses on how a person with CP functions in their life.
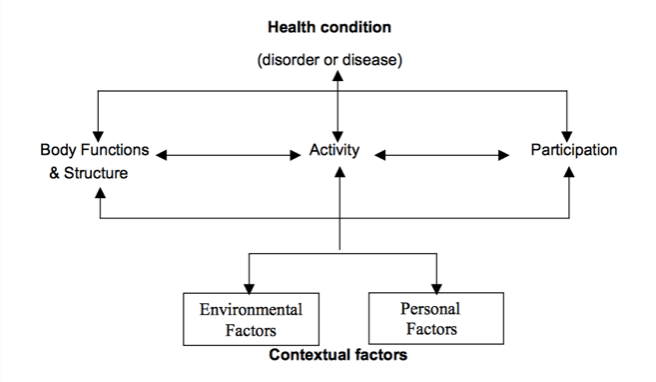
The framework describes three levels of human functioning and characterizes disability as difficulty functioning at one or more of these three levels:
- Body functions and structure refers to functioning at the level of the body or a body part. Spasticity is at this level. Impairments are problems in body function or structure, such as a significant deviation or loss.
- Activity is the execution of a task or action by an individual. Is the person able to walk or kick a ball? Activity limitations are difficulties an individual may have in executing activities. To meet the latest (2007) definition of CP, a permanent motor disorder has to cause activity limitation.
- Participation is involvement in a life situation. Being able to play sports with friends or having a job are examples of participating in society. Participation restrictions are problems an individual may experience with their involvement in life situations.
The framework also includes factors that influence any of the three levels of functioning (termed contextual factors):
- Environmental factors make up the physical, social, and attitudinal environment in which people live and conduct their lives. Examples of physical environment include structural barriers at home and in the community, such as steps or stairs without handrails in the house or a school building with stairs but no elevator.
- Personal factors include gender, age, coping style, social background, education, profession, past and present experiences, and other factors that influence how disability is experienced by the person. Examples of personal factors include a person’s attitude, determination, motivation, and perseverance.
The three levels of human functioning, plus environmental and personal factors, are all interconnected with the health condition.
With regard to activity, the ICF distinguishes between motor capacity—what a person can do in a standardized, controlled environment, and motor performance—what a person actually does in their daily environment. For example: is the child walking at an appointment on a smooth surface with the medical professional and parent watching and encouraging them the same as their walking in a crowded playground on possibly uneven surfaces?
There is a third concept to keep in mind when considering activity: motor capability—what a person can do in their daily environment. For example, a child may be able to ride a bike to school—they have the capability—but they may choose not to. Their performance is influenced by their choice. Holsbeeke and colleagues (2009) noted that physical and social environment and personal factors such as motivation influence the relationship between capacity, capability, and performance.
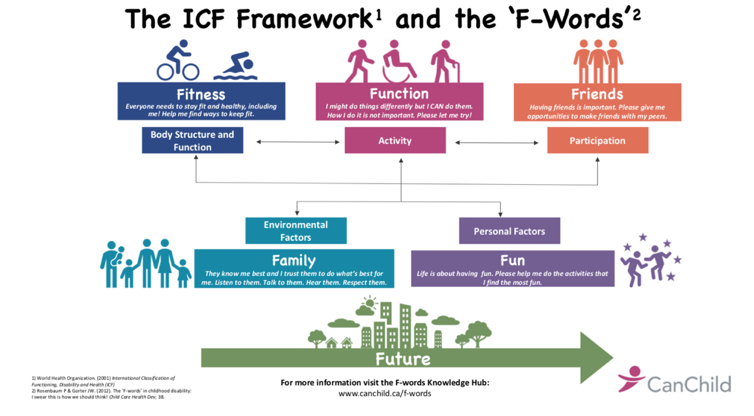
A series of “F-words” have been developed by Rosenbaum and Gorter (2012) and inserted into the different areas of the ICF, providing a useful adaptation of the framework. The authors highlighted fitness, function, friends, family, fun, and future as areas of focus for the child with a health condition. Indeed, these also apply to adults. Web links to a number of useful videos on the F-words are included at the end.
I’ve observed how becoming familiar with the ICF has influenced my thinking over the years. In the early days, I was very focused on issues at the “body functions and structure” level. Later I came to understand the relationship between the three levels. For example, orthopedic surgery leads to improvements at the level of body functions and structure by addressing muscle and bone problems. As a result, the child may walk more easily and their walking might consume less energy. This is an improvement at the “activity” level. If walking is less tiring, the child might be able to keep up and do more with their peers—an improvement at the “participation” level. I also came to understand that treatments need to benefit a child at the level of activity and/or participation rather than purely at the level of body functions and structure. It is important to keep in mind that one cannot assume that a treatment at one level will necessarily help the child at another.
Useful web links
- CanChild (2019) The ICF for Parents (P-ICF). (online) (Scroll down the page for a very useful video series on the ICF.)
- Cerebral Palsy Foundation (2016) The F Words of Disability. (video)
- CP-NET (2018) My Favourite Words. (video)
- CP-NET (2015) These Six F-Words Won’t Fill up Your Swear Jar: What Do the F-Words Mean to Youth with Impairments? (video)
The above is an extract from Spastic Diplegia–Bilateral Cerebral Palsy available here.